guide
Everything you need to know about prior authorization in 2025

What is prior authorization, and why is it needed?
Prior authorization (PA) is the way for payors to determine medical necessity before care is delivered. When appropriately used, prior authorization should lead to better care and ensure that the proper treatment is provided at the right time.
Prior authorization reduces waste from duplicative or unnecessary procedures, while helping to control premiums. Think of it as a guardrail for evidence‑based medicine, not an enemy of clinicians.
Unfortunately, today’s PA process operates with fragmented rules, paper‑era workflows, and endless phone/fax loops that slow down care.
How prior authorizations became so painful
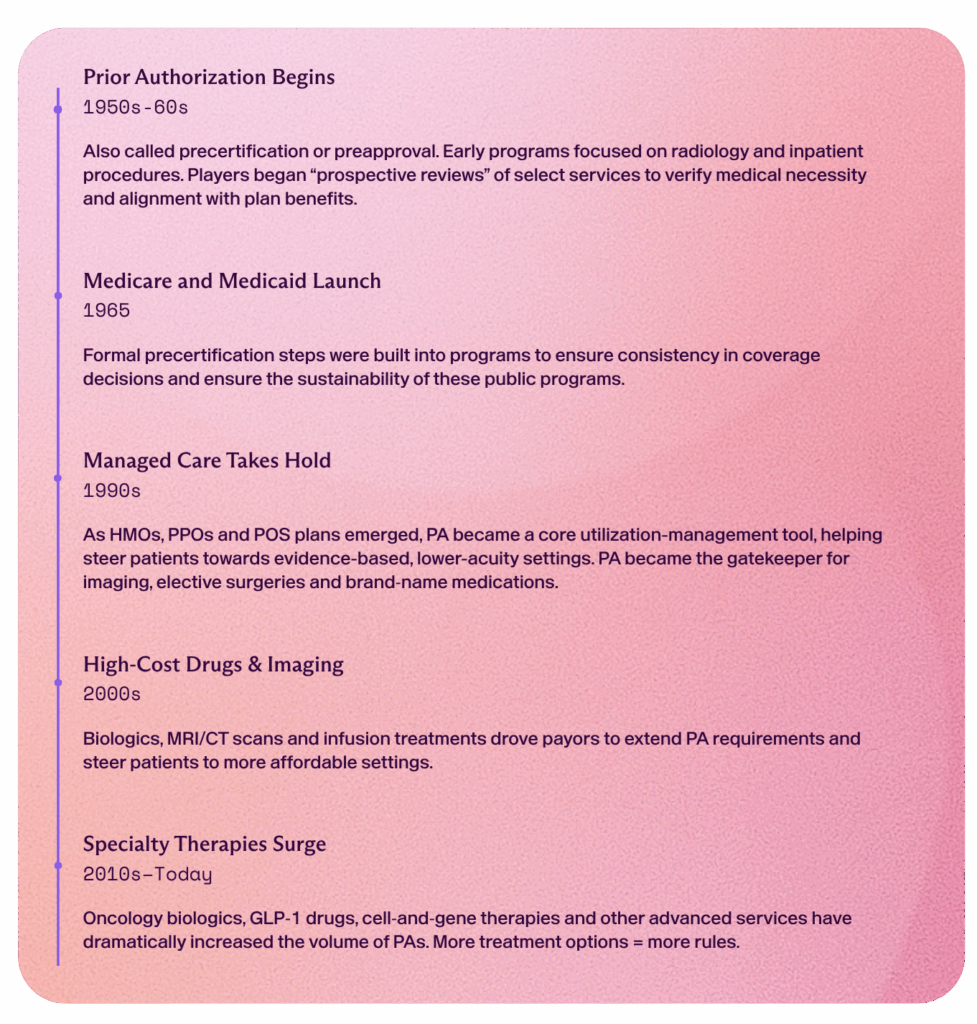
History of prior authorization
Why prior authorization is broken
Innovation in care causes complexity in coverage.
Breakthroughs in medicine have transformed patient care, but they’ve also created more coverage pathways. As GLP‑1 drugs, gene therapies, biologics, advanced imaging, and digital‑health tools emerge, payors must constantly update clinical criteria within disjointed systems, making it impossible to pinpoint the right service under each member’s benefit plan. Consequently, prior authorization has proliferated as a tool to verify medical necessity, determine the optimal care pathway, and ensure alignment with each plan.
Manual friction leads to delays and resource drain.
Disconnected portals, phone-and-fax handoffs, and manual prior-authorization workflows turn minutes of review into days or even weeks, bogging down providers and payor teams with endless eligibility checks and PAs. This leads to:
- Delays: Weeks‑long approvals leave patients waiting and sometimes missing doses.
- Chase mode: Clinical and billing staff spend hours tracking down faxes and making calls.
- Resource drain: Clinicians are having to provide more supporting documentation, which leads to an administrative burden, less time for patient care, and a higher risk of errors in records.
A cost‑control mechanism now costs us time, money, and goodwill. Reform is about restoring its purpose through intelligent automation.
The reform arc we’re entering

Change is underway. Payors are pledging to cut low‑value PAs and publish turnaround metrics. CMS has mandated faster, electronic responses. Providers are adopting technology that automatically detects requirements, submits clean requests, and tracks responses in real time.
CMS is even piloting AI reviews in new categories. The prior authorization process is rapidly evolving, and now is more critical than ever to understand the new requirements.
01. WISeR Model—Medicare pilot for new PA requirements
On June 27, 2025, CMS unveiled the Wasteful and Inappropriate Service Reduction (WISeR) Model. WISeR is a tech‑driven pilot for prior authorization and early claims review across 17 service categories.
- When and where: Effective January 1, 2026–December 31, 2031 in NJ, OH, OK, TX, AZ & WA
- Why: CMS selected these services because they are vulnerable to fraud, waste, or inappropriate use.
- How: Reviews will be conducted by technology companies (using tools such as AI), rather than by traditional Medicare administrative contractors.
- Submitting: Providers can choose to submit a PA through their Medicare Administrative Contractor (MAC) or directly with the tech vendor. If providers skip the PA, the claims will be subject to post-service medical review.
- Exclusions: Inpatient-only services, emergency services, and services that would pose a substantial risk to patients if substantially delayed.
View the full list of WISeR procedure categories and codes:
02. 2024 CMS Interoperability and Prior Authorization Final Rule
In January 2024, CMS issued the Interoperability and Prior Authorization Final Rule (CMS-0057-F), requiring payors to adopt the HL7 FHIR standard and implement a Prior Authorization API. Key mandates include:
By January 1, 2026, impacted payors must:
- Return PA decisions within 72 hours for urgent requests, and 7 calendar days for standard.
- Provide clear reasons for PA denials.
- Publish PA approval and denial rates, appeal outcomes, turnaround time, and all medical items/services requiring PA.
By January 1, 2027, impacted payors must:
- Implement an API that lists covered services, required documentation, and returns approvals/denials with reasons and end dates. Payors may use FHIR only or a combo of FHIR and X12 standards.
If you are a MIPS-eligible provider:
- Eligible clinicians must attest to submitting at least one electronic prior authorization using a FHIR‑based API using CEHRT in 2027 (affecting CY 2029) to stay MIPS‑compliant.
This rule promises quicker decisions and fewer manual steps if providers integrate with these APIs.
03. Growth of state and payor‑level “gold card” exemptions
As of July 2025, five U.S. states—Texas, Arkansas, West Virginia, New Mexico, and Louisiana—plus UnitedHealthcare (UHC) and Humana have implemented gold card prior authorization exemptions. Providers with an approval rate of greater than 90% for a service can earn a gold card and skip the PA process for that service. It’s basically a trust badge for “high-performing” providers.
- How it works: Payors review historical approvals. If a provider meets the threshold (typically 90%), they are exempt from PA for specific procedures for a limited time. The card is subject to periodic review.
- Why it matters: If you are deemed a high-performing provider by a payor, it results in fewer prior authorization requirements from the payor. Investing in the PA process leads to less administrative work required for your practice.
04. Convergence of regulation and technology
2025 is an inflection point. CMS mandates are being phased in. Large language model platforms (e.g., OpenAI, Anthropic) have achieved human-level coding accuracy. These models can extract CPT/ICD codes, auto‑populate forms, track expirations, and predict denial risk.
- CMS milestones: Decision turnaround requirements, FHIR APIs, and public reporting start taking effect in 2025–2026.
- AI milestones: AI reaches human-level accuracy, performing on par or exceeding the accuracy of seasoned coders.
05. Labor pressure and denials intensify
The Association of American Medical Colleges projects a shortfall of up to 86,000 physicians by 2036. Meanwhile, commercial payors denied $1 of every $10 billed in 2024. With staffing caps and rising denials, manual insurance workflows simply won’t scale. Providers need to find efficiencies in their practices.
The financial and human cost of manual PA
Daily burden
Policy updates and AI promises sound abstract until you’re juggling dozens of prior auth tasks each day: schedulers scanning multiple portals for the correct form, nurses racing to fax charts and lab reports, billing staff calling insurers back-to-back to check status, and clinicians pulling detailed clinical notes to justify every line item.

Meanwhile, every re‑submitted request requires re‑keying patient demographics and benefit info—often with minor tweaks to meet each payor’s unique template. The result? A mounting stack of unprocessed requests, missed clinical windows, overtaxed teams stuck in phone‑tag loops, and patients left waiting on hold for answers. The result isn’t just inconvenience—it’s burnout, lost revenue, and poor patient outcomes.
Let’s examine the actual human and financial costs. In 2024:
- Total medical spend tied to PA admin work was $1.26 billion in 2024. (CAQH 2024 Index)
- Initial claim denials hit 11.8%, up from 11.5% the prior year (Healthcare Finance News).
- Denials due to human error: 46% of claim denials are primarily caused by missing or inaccurate information, e.g., data entry, codes, etc. (Experian State of Claims 2024)
Human Toll & Patient Risk
According to the AMA 2024 Prior Authorization Physician Survey:
- 93% of physicians say prior authorizations delay necessary care.
- 29% have seen a life-threatening or serious adverse event tied to delays.
- 82% of clinicians report that patients abandon treatment because of PA complexity.
- 89% say PA contributes to physician burnout.
Ripple effect: Slow scheduling drives patients away, turnover increases retraining costs, and hundreds of thousands go unbilled, causing satisfaction to plummet and eroding your competitive edge.
From bleeding resources to predictable revenue
Stop denials before they happen.
Most denials are preventable. They stem from data accuracy issues, not clinical disputes. Eligibility gaps, poor data quality, and missing information delay care and lead to lost revenue. Automation isn’t optional; it’s mission‑critical to keep care flowing and your margins healthy.
What AI-powered prior auth actually looks like
AI-powered prior authorization software increases data integrity at the source. With revenue cycle automation, accuracy and speed are no longer a trade-off. AI can:
- Catch errors before submitting a prior authorization.
- Manage end‑to‑end automation of form submission, response tracking, and follow‑ups.
- Flag high‑risk cases based on historical patterns and payor policies to prevent denials.
Critical prior auth metrics to track
| Metric | Target/Signal | Why It Matters |
| Submission time | 20 minutes | Faster scheduling leads to faster responses, happier patients, and fewer cancellations |
| Denials tied to auth/eligibility errors | Less than 1% | Protects your bottom line and reduces rework |
| Labor hours/FTE on insurance workflows | Decrease 50–80% | Redeploy staff to higher‑value work |
| First‑pass denial rate | Trending down quarter‑over‑quarter | Clean cash flow, fewer appeals |
| Patient collections vs. refunds | Collections up, refunds down | Accurate out‑of‑pocket estimates reduce write‑offs |
The future of prior authorizations
The prior authorization landscape is evolving rapidly. With AI reaching human‑level accuracy, providers can focus on patient care while automating administrative tasks. Imagine a world where:
- Authorizations are secured before every visit.
- Staff focus on patients, not portals.
- Denials are less than 1%, and follow‑ups happen automatically.
The result? Patients receive timely care, staff are happier, and the business grows.
Ready to move from paperwork to patient care?
Silna handles all prior authorizations, benefit checks, and insurance monitoring upfront to make sure your patients are clear to receive care, and you have more capacity to provide it.
Want more information on CMS rules, the WISeR pilot categories and codes, and the future of PA? Download the complete whitepaper.
FAQs
What are the new CMS prior‑authorization deadlines for 2026?
▼
CMS requires impacted payors to return decisions within 72 hours for urgent requests, and seven calendar days for standard requests.
How does AI reduce prior‑authorization denials?
▼
AI tools validate requirements, auto‑populate accurate data, and predict denial risk so submissions are clean and complete.
Will AI‑PA tools comply with FHIR‑based PA APIs?
▼
Leading platforms—including Silna—connect directly to payor FHIR endpoints, enabling real‑time status updates and document retrieval.
Does AI replace staff?
▼
No. Automation creates leverage in an organization so that their team can focus on the most critical part of their job: ensuring top-tier patient experience and care.
What is a prior authorization gold card/gold carding?
▼
A “gold card” (or “gold carding”) means a payor exempts a clinician or facility from PA for certain services. It’s awarded when a provider hits a specific approval rate. It’s basically a trust badge for “high-performing” providers.
How are gold cards earned?
▼
Gold cards are typically awarded based on a threshold of requests with at least 90% approvals for a specific service. Gold cards are time-limited and re-evaluated periodically.